
Day One Highlights: The Patient Engagement Solutions & Innovation World Congress
- Olivia Kersey

- Apr 1
- 5 min read
This first event of its kind provided an opportunity to explore and question the evolving role of technology in research and care and how this may influence the future of patient engagement.
“Done beats perfect” — examining cultural barriers to progress
In the opening panel, Rasmus Hjorth of James Lind Care spotlighted something most organisations know but rarely say out loud: the tendency to wait for a complete strategy before taking (even small and safe) actions. His point wasn’t to encourage sloppiness; it was that the pursuit of the perfect framework can itself become an obstacle. What the field needs is people willing to act on imperfect information and recognise the balance between preparedness and paranoia to transcend counterproductive immobilisation.
Another key observation from Hjorth: when evaluating new technologies, the right first question is “What are we substituting – and why?” Rather than asking what a tool can do, ask what it replaces. That reframing catches assumptions that forward-looking enthusiasm tends to skip over.
Later, Keith Berelowitz, Founder and CEO, pRx Engage, called for greater collaboration between patient organisations, noting there can also be a tendency towards siloed working in those settings as well as in industry.

“Critical friends” and the urgency of trial design innovation
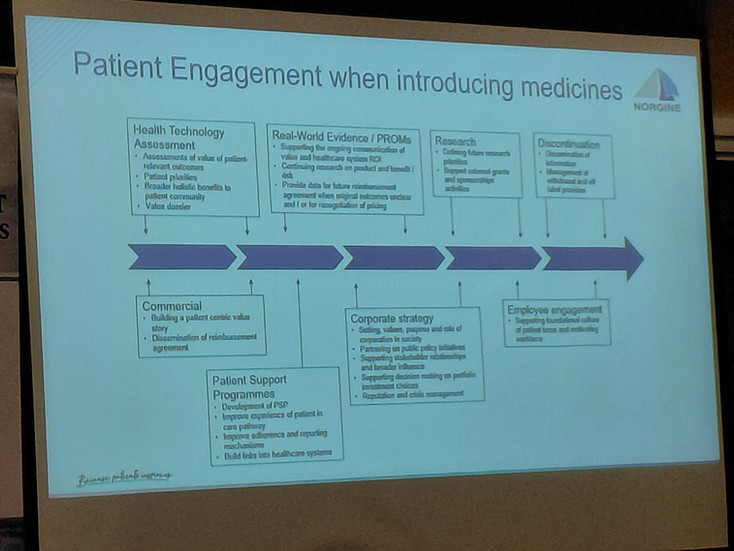
David Gillen, Chief Medical Officer at Norgine, gave one of the more candid presentations of the congress. He spoke directly about commercial incentives and what he called the “critical friend model” – his preferred framing for how pharma should relate to patient organisations.
The argument was precise: not friendship, not entanglement, but a respectful relationship that can survive difficult moments. His reasoning was practical. When things go wrong – and in drug development, they do – organisations need relationships that were built on something more durable than enthusiasm. Physicians who had been closely aligned with pharma, he noted, largely disappeared when challenges arose. Patient organisations are not immune to the same dynamic if relationships aren’t built sustainably and transparently from the start.
The conversation then moved to the need to balance scientific integrity with ethical duty; for example, mitigating the need for control data while not restricting access to novel treatment in critically urgent cases such as advanced paediatric cancer. Patient Affairs specialist and ISPEP team member Olivia Kersey commented, “We need statistical experts to translate our scientific and ethical concerns about control arms into viable alternative models for trial design.”



Five hospitals, 21 clinicians, zero unified records
Hannah Humphrey, lived experience expert and parent of a child with multiple conditions, gave a precise account of what fragmented healthcare systems look like in practice. Her daughter Tabby is cared for by 21 healthcare professionals across five hospitals; appallingly, none of the electronic records systems are unified. Hannah described her role as the “human bridge” between those systems – carrying clinical information between providers who cannot see each other’s notes, and managing the risk that critical details will simply not be visible at the point they’re needed.
"This isn't empowerment. This is risk displacement. The burden is shifted is from the system to the caregiver, and the system quietly assumes that we'll always be there to capture anything that falls through."
The point she pressed was not that digital systems are inherently bad but that they were not designed with families like hers in mind. Her ask was specific: involve the people who carry the information burden in designing the systems meant to replace it.
What empathy-led trial support actually looks like in practice
Next up, mdgroup presented two case studies to demonstrate what meaningful support of trial participants can look like.
The first involved a medically fragile six-year-old boy in the UK with a rare developmental condition. The trial he was enrolled in was not approved within the UK, requiring the family – two working parents, a breastfeeding infant sibling, and a child with significant care needs – to travel to the EU for each visit. The response was a full pivot to a decentralised model: the trial was redesigned around the family. Travel was planned around seizure triggers; flight times were kept under an hour; the family arrived to a fully prepared home near the trial site. Home visits included investigational product delivery and administration, eight hours of blood sampling, full neurological and physical exams, ECGs, and real-time telehealth connection to the principal investigator. The point made was not that this was operationally impressive – though it was – but that empathy-led planning eliminated barriers before they had a chance to become dropout events.
The second case involved adult ALS patients in a global Phase 2 trial. ALS is not linear: mobility, speech, swallowing, and respiratory function can all shift within the timeframe of a single trial, transforming what participation means month to month. The model mdgroup used prioritised adaptability above all else: a mix of site and home visits, flexible scheduling, nurse continuity (most patients had one dedicated nurse), and the option to follow patients wherever they were – including on holiday. When patients died during the trial, the relationships built with caregivers were strong enough that mdgroup team members were able to return to collect patient diaries and leftover study drugs, removing a logistical burden from families at an already hugely overwhelming time.
The principle underlying both cases was stated plainly: when research is designed around the whole person (and their loved ones) rather than the protocol, complex requirements become achievable.
Digital coaching for brain tumour patients: the Brainstrust model
Brainstrust, a national charity supporting brain tumour patients, presented their Thrive platform – an on-demand coaching service delivered via video, phone, and chat that supports over 5,000 patients annually. The platform was born of necessity: during COVID-19, immunocompromised patients needed continued support without the option of in-person contact, and the shift accelerated the development of infrastructure that has since proven its value beyond the pandemic context.
The design of Thrive reflects the specific cognitive and sensory challenges that brain tumour patients face. A progress tracker measures impact and allows services to adapt over time. The platform supports caregivers as well as patients, and has extended to include services such as hypnotherapy and AI coaching. Real-life cases presented showed measurable improvements in emotional resilience and quality of life. The model is a useful example of a digital platform that started from patient need rather than technological capability – a distinction that comes through in both its design and its outcomes.








Day One closing panel: preserving humanity in digital health
The closing panel for Day One, moderated by Olivia Kersey (ISPEP), brought together Lisa Kerr (Evinova), Keith Berelowitz (pRx Engage), Hannah Humphrey (Lived Experience Expert), and Derick Mitchell (PFMD) to examine the tension between digital integration and human connection in care delivery.
This rich dialogue has been covered in detail in a dedicated, separate article on the ISPEP Hub: Compassionate Convergence of Man and Machine: Preserving Humanity in Digital Health. With topics covered including the “simulated empathy” of AI chatbots, the disconnect between industry innovation and burden at ground level, and unmet needs regarding accessibility and transparency, this candid discussion is not one to miss.

Watch this space for highlights from Day Two – coming soon to the ISPEP Hub.
Comments